A blog for humans in the universe, to understand what we know now and to imagine what we don't know. To bridge the gap between the real world, its image in our brain and the ideas generated by.
It was with this background that studies of BCG in bladder cancer began. Studies by Coe and Feldman 17 in 1966 showed that the bladder responded to BCG with a delayed type hypersensitivity reaction seen with the skin, and in 1974, Silverstein et al. 18 reported response of melanoma metastatic to the bladder treated with intralesional BCG. This success in melanoma led, at the suggestion of David McCullough, to the evaluation of BCG in an animal model of bladder cancer 19. At the same time, Morales independently began clinical studies and in 1976, published results of the first successful clinical trial of intravesical BCG administration in nine patients with recurrent bladder cancer.
The original BCG protocol was initially conceived by Morales in 1972 20. A Canadian urologist, Morales obtained the BCG strain manufactured by the Montreal Institute Armand. Morales knew that, to establish a delayed hypersensitivity reaction, a minimum of 3 weeks of treatment was necessary and would be gauged by an intradermal BCG injection. Additionally, he had determined that adverse effects resolved within 1 week, prompting a weekly schedule. The Armand Frappier vaccine was packaged as 120 mg each dispensed in six separate vials, therefore establishing a six weekly bladder instillation protocol. The results of that study found six weekly intravesical plus percutaneous administrations to result in a 12‐fold reduction in bladder tumour recurrence 21.
This success prompted the National Cancer Institute to request proposals for controlled human clinical trials using Morales' technique and contracts were given to Lamm at the University of Texas in San Antonio and Pinsky at Memorial Sloan‐Kettering Cancer Center (MSK) in New York. The initial BCG controlled trial, published in 1980, showed statistically significant reduction in tumour recurrence in 54 evaluable patients 22 and showed an advantage that increased with time 23. Similar results were reported in much higher risk patients in the MSK study 24. Subsequent follow‐up of these patients suggested that the benefit of a single 6‐week course of intravesical plus percutaneous BCG provided long‐term protection from tumour recurrence and even reduced disease progression. However, the 15‐year follow‐up of the MSK series showed the limitations of BCG protection without initiation of maintenance therapy. While induction BCG (six weekly instillations) reduced recurrence, progression and mortality at 10 years, this advantage was lost by 15 years, and patients remained at high risk for progression and the development of disease in the prostatic urethra (24%) and upper tracts (25%). A mortality rate of 32% was seen in patients with disease progression into the upper tracts and in 44% of those with prostatic urothelial disease 25.
BCG Immunotherapy Technique in Bladder Cancer
Immune Response to BCG
It is often said that the true mechanism of action for BCG is unknown. In fact, a great deal is actually known about the immune response to BCG. As a complex living organism, the responses induced to BCG infection are broad and highly varied. BCG attaches to bladder tumour cells as well as urothelial cells by means of specific fibronectin and integrin receptors 26, 27. Internalization of BCG is correlated with immune response and sensitivity to BCG. In vitro studies suggest that poorly differentiated cell lines internalise BCG and are sensitive to it 28. Clinical studies similarly suggest that low‐grade tumours are relatively less sensitive to BCG 29. Antigens specific for BCG are expressed on the surface of tumour cells and MHC class II antigen expression is upregulated 30-32.
BCG is a nonspecific stimulant to the reticuloendothelial system and induces a local inflammatory response with the infiltration of granulocytes followed by macrophages and lymphocytes, particularly helper T cells. Phagocytosis and the ratio of helper/suppressor cells are increased 33. A wide range of cytokines are induced, including interleukin (IL)‐1, IL‐2, IL‐6, IL‐8, IL‐10, IL‐12, TNF‐α, interferon (IFN) γ, granulocyte/macrophage colony stimulating factor and soluble intercellular adhesion molecule I 34. The cellular immune (Th1response) predominates and is correlated with tumour destruction.
Recent studies show that BCG, like other mycobacteria, contains high amounts of CpG oligodeoxynucleotide motifs, known to induce TNF‐related apoptosis‐inducing ligand (TRAIL) by IFN production. After BCG administration, the cytokine response induces TRAIL up‐regulation. Urine IFN and TRAIL levels were initially undetectable in BCG therapy patients but subsequent treatments led to identification of TRAIL and TRAIL‐expressing neutrophils in the urine and this expression was correlated with response to BCG therapy 35.
BCG in Bladder Carcinoma in situ (CIS)
Animal studies have shown that effective BCG immunotherapy requires an immune competent host, an adequate dose of BCG, juxtaposition of BCG and tumour cells, and a limited number of cancer cells. These conditions are optimally met in bladder cancer, especially CIS. In 1980, Morales 36 reported a 71% complete response rate in patients with CIS of the bladder using a 6‐week BCG induction. BCG (Theracys) was initially approved by the USA Food and Drug Administration for bladder cancer in 1990 based upon its demonstrated superiority (71% complete response, 48% disease free at 5 years) over doxorubicin (47% complete response, 18% disease free at 5 years) in the treatment of CIS 37. The consistency of the efficacy of BCG in CIS is noteworthy, regardless of strain utilised (Table 1). Complete responses were seen with every strain of BCG despite variations in dose and schedule, and the 70% response rate is remarkably consistent 38. One controlled study provides important clinical information in the management of CIS. The Southwest Oncology Group (SWOG) study of 6‐week induction followed by 3‐week maintenance BCG vs standard 6‐week induction without maintenance included 269 randomised patients with CIS. An increase in complete response (58% at 3 months to 68% at 6 months) was seen in the induction‐only arm, suggesting that while residual CIS is a poor prognostic feature, it may take up to 6 months for the full complete response to occur. With three additional weekly BCG maintenance instillations beginning at 3 months, 64% of those with residual CIS at 3 months had resolution at 6 months, yielding an overall complete response rate of 84% 39. With continued 3‐week maintenance BCG after 3 months, >70% of patients with an initial complete response remained tumour‐free for >5 years; a remarkable achievement considering that series historically reported progression in 54% of patients with CIS within that same timeframe 40.
Table 1. Comparison of BCG strains in the treatment of CIS of the bladder 38.
Strain/series
Total number
of patients
Complete
responses, n
Complete
response rate, %
Range of
response rates, %
Connaught/8
450
357
79
70–92
Tokyo/4
111
86
77
63–84
Pasteur/7
230
171
74
40–80
Tice/6
277
197
71
56–82
Evans/6
180
117
65
53–88
A. Frappier/6
145
87
60
39–100
S. African/1
13
9
69
–
Danish/1
42
28
67
–
Romanian/1
33
21
64
–
RIVM/1
15
9
60
–
Total
1496
1082
72
39–100
Maintenance BCG, Disease Progression, and Mortality
It is generally accepted that induction BCG is highly effective in reducing disease recurrence, but controversy persisted about the role of maintenance BCG and its ability to reduce disease progression and mortality. Lamm 41 initially reported a four‐fold reduction in the rate of tumour recurrence in patients treated with quarterly single BCG instillations. A controlled evaluation in 1987 of this regimen in 42 patients failed to show a significant reduction in tumour recurrence 42. In the same year, Badalament et al. 43 reported a randomised study of 93 patients comparing 6 week induction with monthly maintenance BCG and found no significant benefit for maintenance therapy. These studies could be criticised for their relatively short follow‐up and lack of power, but nevertheless, they had a major impact on clinical practice. As it stands today, the benefit of maintenance BCG and the optimal schedule continue to be questioned 44. Many urologists have adopted an initial 6‐week BCG induction course followed by a repeat 6‐week cycle at the time of tumour recurrence, despite absence of randomised clinical trials supporting this approach. Palou et al. 45 found that 6‐week maintenance BCG every 6 months for 2 years was not significantly better than induction alone in a study of 126 patients with CIS followed for an average of 79 months.
Despite these ‘negative’ studies, maintenance therapy may be the most important advancement in BCG treatment of bladder cancer since the introduction of Morales' original 6‐week induction regimen. Maintenance immunotherapy is vital, all while balancing the administration of excessive BCG to prevent causing immunosuppression. The risk of tumour recurrence and disease progression is life‐long in most patients, but the immune stimulation induced by BCG wanes with time. A controlled trial of 384 patients using an immunologically sound maintenance schedule (intravesical and percutaneous BCG each week for 3 weeks given at 3, 6, 12, 18, 24, 30, and 36 months) clearly showed that 3‐week maintenance BCG markedly reduced long‐term recurrence and disease worsening 39. While other, presumably inferior, maintenance schedules have not achieved statistical significance in randomised controlled trials, a meta‐analyses showed that induction + maintenance BCG is superior to induction BCG alone and may be required for the most important benefit of BCG – the reduction of tumour progression 46.
A 6‐week induction course induces a prolonged protection from tumour recurrence and may help explain the failure to show a benefit of maintenance studies with short follow‐up. In animal studies, no benefit of BCG maintenance was seen at 9 months, but a highly significant benefit was documented at 15 months 47. In Herr's 25 series, a significant reduction in tumour recurrence, disease progression, and mortality persisted for 10 years, but was no longer significant at 15 years. This is in agreement with the initial finding of 10 year conferred protection from the MSK series 24. The SWOG maintenance study of 384 evaluable patients (up to three weekly instillations at 3, 6, 12, 18, 24, 30 and 36 months) found a highly significant reduction in tumour recurrence (P < 0.001), as well as a significant reduction in disease worsening (P < 0.04), defined as stage progression or the requirement for cystectomy, radiation therapy, or systemic chemotherapy 39.
In the meta‐analysis by Bohle et al. 48, all six comparison studies using maintenance BCG schedules found BCG to be clearly superior to mitomycin C (MMC), while only one study reported statistical significance in groups not using maintenance BCG. However, the most convincing data is in the meta‐analysis published by Sylvester et al. 46. In that analysis of 24 studies comprised of 4863 patients, BCG was compared with surgery, chemotherapy, or other immunotherapy with endpoints of disease progression and cancer‐specific mortality being investigated. Disease progression was found to be significantly reduced by 37% (P < 0.001); however, this benefit was only seen in patients receiving maintenance BCG. Bladder cancer mortality was reduced by 19%, but statistical significance was not achieved (P = 0.20) due to the short median follow‐up of only 2.5 months. Malmström et al.49 analysed nine randomised trials comparing the long‐term efficacy of intravesical MMC against BCG (induction alone and with maintenance) with time to first recurrence as the primary endpoint. BCG maintenance was found to confer a 32% reduction in the risk of recurrence for BCG compared with MMC, producing a statistically significant 4% difference against trials without BCG maintenance (P < 0.001). It was determined that for prophylaxis against recurrence, BCG maintenance was required to achieve the demonstrable superiority over MMC.
Subsequent randomised clinical trials have shown that the 3‐week, 3‐year maintenance schedule used by the SWOG has achieved success that dwarfs that of other intravesical treatments. In a European study of 957 patients with intermediate‐to‐high risk urothelial carcinoma without CIS, the 3‐week maintenance schedule was compared with intravesical epirubicin chemotherapy using the same schedule. The 3‐week maintenance BCG regimen significantly decreased recurrence (P < 0.001), metastasis (P < 0.046), and improved overall and disease‐specific survival (P < 0.023) 50. In a subsequent study assessing 3 years of BCG maintenance against 1 year maintenance therapy while maintaining a 3‐week instillation schedule, full dose 3‐week maintenance for 3 years significantly reduced recurrence compared with one‐third dose BCG maintenance for 1 year 51.
BCG Toxicity
Most patients tolerate BCG well, but as with most cancer treatments, serious and potentially fatal toxicity can occur 52. Irritative bladder symptoms (frequency, dysuria, low‐grade fever) typically can begin after the second or third instillation and last for 1–2 days as a result of immune stimulation and cytokine production. These symptoms may be associated with a more favourable anti‐tumour response to BCG 53. Severe reactions or infection with BCG result from i.v. absorption of the organism, most commonly from traumatic catheterisation. While BCG sometimes is given in the presence of haematuria, blood arising from a difficultly placed catheter is an absolute contraindication to instillation of BCG. Patients with continuing symptoms from earlier BCG administrations are best treated with antibiotics rather than forging ahead with more BCG. Logarithmic dose reduction of BCG in patients with increasing side‐effects will typically prevent escalation of toxicity. While the use of fluoroquinolone prophylaxis has been shown to decrease the incidence of moderate‐to‐severe BCG‐related adverse side‐effects 54, there were no differences in local or systemic adverse reactions after prophylactic administration of isoniazid anti‐tubercular medication 55. Patients with BCG sepsis require steroids in addition to gram negative and anti‐tubercular antibiotic therapy to reduce the severe hypersensitivity component that can otherwise prove fatal. As the risk for bacterial sepsis and possibly death is high, BCG should never be used as an immediate postoperative intravesical instillation.
BCG Comparisons with Intravesical Chemotherapy
The successful demonstration that BCG reduced tumour recurrence compared with surgery alone was followed by many controlled comparisons of BCG vs intravesical chemotherapy. As shown in Table 2, BCG was uniformly found to be better than chemotherapy with thiotepa, doxorubicin, and MMC 56. However, comparisons with MMC have shown an inconsistent advantage for BCG. The AUA management guidelines for NMIBC, recently validated in 2010, listed immunomodulator agents (BCG, IFN) and chemotherapeutic agents (thiotepa, MMC, doxorubicin, gemcitabine) as beneficial intravesical therapies. The guidelines state BCG has become a first‐line treatment for CIS, and that both BCG and MMC are effective in prophylaxis against tumour recurrence 57. A SWOG study comparing six weekly instillations of either BCG or MMC followed by monthly instillations for 1 year showed the 3‐year benefit in tumour reduction with use of BCG over MMC, prompting early termination of the study (Fig. 1) 58.
Study comparison between BCG and MMC for bladder tumour recurrence 58.
Table 2. Overview of controlled trials of BCG vs chemotherapy for superficial bladder cancer 56.
Median rate of recurrence, %
No. of positive trials
BCG arm
Chemotherapy arm
BCG vs thiotepa
7
42
3/3
BCG vs doxorubicin
38
64
2/2
BCG vs MMC
30
43
3/6
Further work has clearly shown that BCG is superior to MMC in these high‐grade patients. As mentioned earlier, the meta‐analysis of Bohle et al. 48 found maintenance BCG to be significantly better than MMC alone or induction BCG alone.48 In a subsequent meta‐analysis by the Cochrane group, BCG was found to be markedly superior to MMC in high‐risk patients but not in low‐risk patients 59. Additionally, the National Comprehensive Cancer Network guidelines lists the use of intravesical BCG as preferred therapy, citing Category 1 data for high‐grade Ta, all T1, and any Tis tumors 60.
Despite comparisons of BCG and MMC in determining superiority for maintenance therapy, Di Stasi et al. 61 assessed the combination of the two treatment methods in evaluating disease‐free intervals. In looking at 212 patients (105 receiving sole BCG induction + maintenance and 107 receiving MMC + BCG), those treated with both MMC (40 mg electromotive MMC once a month for 2 months) and BCG (81 mg once a month as one cycle for three cycles) as maintenance therapy showed a higher disease‐free interval (difference of 48 months, P = 0.001), lower recurrence (16% difference, P = 0.001), progression (12.6% difference, P = 0.004), overall mortality (10.9% difference, P = 0.01), and disease‐specific mortality (10.6% difference, P = 0.01). There were no significant differences in side‐effect profiles, and the thought is the electromotive delivery of MMC allows for the destruction of malignant cells that may have escaped the immunological activity induced by BCG.
Croire que la criminalité est due à la structure sociale c’est-à-dire à l’existence d’interdits c’est exactement comme croire que la pauvreté est due à l’exploitation de l’homme par l’homme. Encore une fantastique victoire du constructivisme et du marxisme. En réalité dans le groupe humain il y a des individus qui ont un comportement antisocial et violent. C’est vrai aussi des animaux antérieurs dans l’évolution. Compte-tenu du cerveau humain et du type de société que nous bâtissons, ce comportement antisocial est d’abord lié a des éléments neurobiologiques structuraux dont 50-60% sont génétiques.
Les gagnants et les perdants du monde numérique vont dessiner la société de demain, en effet la digitalisation des activités humaines est en cours. Les objets connectés vont progressivement remplacer les objets sans informations numériques sur leur nature et leur fonctionnement. Ces objets connectés sont en réalité des êtres numériques dotés de fonctionalités et communiquant leur données. Toutes les activités humaines vont être impactées par cette digitalisation. La construction, le transport, l’agriculture, la production d’énergie, la médecine etc. C’est un monde où le big data et l'open data permettront de calculer les activités et surtout les externalités négatives.
Les individus resteront libres dans les pays libres mais il se produit déjà une transformation de leur rapport à la société. L’État tel qu’on le connaît aujourd’hui surtout dans les pays où son développement est extravagant, va disparaître. Le calcul des externalités négatives sera essentiel pour le calcul des contreparties afin que la société ne pâtisse pas des activités humaines mais au contraire soit bénéficiaire.
Pour cela la block chain, les monnaies numériques, les transversalités de production vont remplacer le couteux dispositif étatique, rigide est souvent inapproprié dans ses effets redistributifs.
Le plus grand perdant de la digitalisation massive c’est l’État. Toute la sphère étatique va s’effondrer lentement par éviction.
Seul pays au monde où c’est le patient qui décide du degré d’urgence.
Seul pays au monde où on peut rencontrer un médecin sans rendez-vous sont téléphoner sans dossier à n’importe quelle heure du jour ou de la nuit.
Seul pays au monde où le médecin est en fait un interne de première année qui n’a fait aucun stage préalable.
"À mon avis l’attitude des deux gouvernement socialiste celui de Hollande et de Macron au sujet des urgences est volontaire. Le but est de créer une demande infinie pour supprimer la médecine libérale et instaurer un système public où les hôpitaux auront un énorme département de médecine « pour soigner ceux qui ont droit à un accès aux soins pour tout à toute heure et gratuit». Un vrai idéal collectiviste. Inscription dans la constitution. Agitation syndicalopolitique aux urgences. Activité de remplacement des hôpitaux qui n’ont pas ou trop peu d’activité programmée."
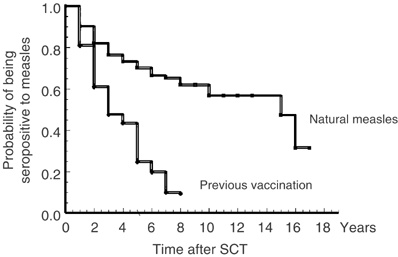
Vaccination could be given at 2 years after transplantation if they did not have chronic GVHD or ongoing immunosuppression.8, 9 Most children have been vaccinated, but only few of the adults have been vaccinated. The indications for vaccination in the adults have been seronegativity in a patient either working with children, having young children in the household, or travel to areas where measles is still endemic."
https://www.nature.com/articles/1704634 Probability of becoming seronegative to measles during follow-up in patients having previously had natural measles disease and in patients having received measles vaccination.
"Among vaccinated patients, Machado et al. (5) observed that 70% had lost measles immunity 3 years after vaccination, suggesting that serological surveillance to check for immunity should be performed in long-term survivors (Table 2). Moreover, the value and the frequency of booster doses of the vaccine should be better investigated in patients who lost measles immunity.
It is important to stress that although most of the recommendations for BMT recipient vaccination are independent of where in the world the patient lives, there are local variations in the scenario of infections that must be taken into account and adjustments in official guidelines are strongly recommended (31). For example, in 1997, hundreds of BMT recipients were exposed to measles when more than 20,000 cases of measles were diagnosed during an outbreak in the city of São Paulo, Brazil. Eight patients acquired measles and early measles vaccination was the strategy used to avoid the appearance of new measles cases among the patients who had lost specific immunity (5)."
This study showed that most adult patients lost immunity to MMR after allogeneic HSCT. Although we did not evaluate the safety and efficacy of vaccination in this study, most HSCT guidelines recommend vaccination for HSCT recipients without active chronic graft-versus-host disease or ongoing immunosuppressive therapy at 24 months after HSCT. Immunization against rubella is especially important for female patients of reproductive age. Further studies will be necessary to evaluate the effect of vaccination on the antibody response in adult allogeneic HSCT recipients.
My conviction is that a trial must be organized as it is clearly crimes against humanity. With the commanders and the organizers and those who brought all the financial support.